Doctorant en sciences de gestion et du management
-
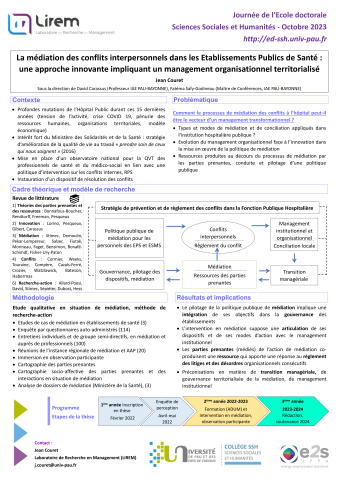
La médiation des conflits interpersonnels dans les Etablissements Publics de Santé : une approche innovante impliquant un management organisationnel territorialisé
- Type de publi. :
- Date de publi. : 19/10/2023
-
Auteurs :
Jean Couret
Fiche détaillée
La médiation des conflits interpersonnels dans les Etablissements Publics de Santé : une approche innovante impliquant un management organisationnel territorialisé
- Type de publi. :
- Date de publi. : 19/10/2023
-
Auteurs :
Jean Couret
-
Organismes :
Laboratoire de Recherche en Management
Fichiers liés :
Présentation_POSTER_Jean Couret.pdf
Source


